Insurance actuaries were the first to notice an unprecedented rise in life
insurance claims among the healthiest sector of society: working-age people with
group life insurance policies. Dr. Pierre Kory writes about the obscene (my
word, not his) suppression of discussion and research on this epidemic of death
“on the scale of a war or terrorist event” in an article in USA Today and a
“longer, less-politically edited version” on Substack. Both essays were
co-written Mary Beth Pfeiffer, who first had the idea and did the original
research.
They write in USAT:
Something other than COVID is causing these deaths. Yet, we see no urgent
response from federal or state authorities like the CDC or NIH or state
departments of health. No interest in identifying what is killing thousands of
people in their prime.
On Substack, (https://pierrekory.substack.com/p/i-published-an-op-ed-in-usa-today?r=p73z9)
they write:
There is much more to see at the Substack version. I can’t begin to tease out
the data myself, but do know that the apparent cover-up of the wave of death is
a scandal and suggests that the authorities who managed the Covid response are
afraid of discovering what the cause really is.
We lost an incredible amount of the freedom we formerly took for
granted when Covid-19 leaked out of a lab in Wuhan, China, and was greeted by
world leaders as a pandemic justifying the radical curtailment of liberty and
enhancement of their own power. Now, they and their lackeys in the academic and
medical establishment see the restoration of those liberties as a threat. George
Washington University Public Health Policy Professor Laura Wen said it out loud
– a classic Kinsley gaffe of accidentally telling the truth about something that
politicians would rather the public not understand. A lot of people noticed,
including Ace of Spades, Legal Insurrection, and Instapundit. This tweet with 38
seconds of video has gotten almost 4 million views:
You can’t have people enjoying freedoms before the government
forces them all to take a experimental drugs, some of which act on their genetic
makeup. One that has caused severe reactions in some, including a number of
deaths.
When people in positions of influence and authority openly bemoan
the restoration of liberty as a lost opportunity for state coercion, they
demonstrate that a new, terrible era is upon us, one of “public health” tyranny.
They pay no taxes and rake in the lion's share of the money from
that nearly $1 trillion a year actual taxpayers spend on Medicaid and Medicare
each year.
On top of that, each of the 82 largest charitable hospitals pay their top
executives more than the president's salary (which Donald John Trump gives back
to the USA.)
Adam Andrzejewski wrote in Forbes magazine in June, "Collectively, $297.5
million in cash compensation flowed to the top paid executive at each of the 82
hospitals. We found payouts as high as $10 million, $18 million and even $21.6
million per CEO or other top-paid employee."
That is an average of $3.6 million per CEO -- or 9 times the president's salary.
He wrote, "Even after paying lavish salaries, these non-profit hospitals had
enough left over to add nearly $40 billion to their bottom-line.
"We found that the assets, investments and bank accounts at these charitable
hospitals increased by $39.1 billion last year – from $164.1 billion to $203.2
billion. That’s 23.6 percent growth, year-over-year, in net assets. Even
deducting for the $5.2 billion in charitable gifts received from donors, these
hospitals still registered an extraordinary 20.5 percent return on investment (ROI).
"In 1970, health care amounted to 7% of gross domestic product (GDP). Today,
estimates suggest the soaring cost of health care will consume 20% of our GDP.
That spending trajectory is unsustainable."
America's tax-exempt hospitals have more money than they know what to do with.
And the are hellbent on keeping it.
Mexican billionaire Carlos Slim's New York Times reported, "The nation’s
hospital groups sued the Trump administration on Wednesday over a new federal
rule that would require them to disclose the discounted prices they give
insurers for all sorts of procedures.
"The hospitals, including the American Hospital Association, argued in a lawsuit
filed in United States District Court in Washington that the new rule 'is
unlawful, several times over.'
"They argued that the administration exceeded its legal authority in issuing the
rule last month as part of its efforts to make the health care system much more
transparent to patients. The lawsuit contends the requirement to disclose their
private negotiations with insurers violates their First Amendment rights.
"The administration wanted the disclosure rule, which would go into effect in
2021, to allow patients to better shop for deals on a range of services, from
MRIs to hip replacements."
Hmm.
The hospital cafeteria must disclose how many calories are in a meal, but
hospitals don't have to disclose their prices. The hospitals argue that this
violates their First Amendment rights.
The lawsuit said, "Under any potentially applicable level of First Amendment
scrutiny, [the government] must show that the mandated speech directly and
materially advances a substantial government interest and that the means chosen
are narrowly tailored to avoid burdening more constitutionally protected
activity than is necessary."
Mandated speech.
That is the best these $1,000-an-hour lawyers can come up with?
This is a tortured argument that makes me long for a Scalia to mock the hell out
of the plaintiff.
These hospital oligarchs fear a price war fueled by posting prices will cut into
that $40 billion a year in profits they make.
Of course. That is the whole purpose of making them say in advance how much the
MRI will be. As tax-exempt non-profits, they are not supposed to make any
profit.
What a dastardly thing to do.
From the Washington Post:
It is hilarious.
These bozos -- global warming dotard Juliet Eilperin wrote the piece -- are
bellyaching because Trump is making people live under this perfect plan they
came up with.
And the Washington Post and the other cheerleaders in the press are just as
culpable because they allowed Obama to lie about 47 million people being
uninsured (the number was half that and most of those people did not want it),
to lie about premiums going down an average of $2,500 per family, and to lie
about keeping your doctor.
Now Eilperin, the Post, and every other Marxist in the nation is stuck with
Obamacare.
President Trump is making them live with its worst parts.
And still they lie.
Those are not cost reductions.
Those are price subsidies.
Eilperin does not know the difference between price and cost.
And nothing in the price is reduced. Trump is stopping taxpayers from having to
pay for someone else's premium.
CNBC latched onto Trump taking action:
That is his job.
His call.
Washington reporters are so used to the unseen bureaucrats making these calls
that it is shocked when a real executive steps up and makes a decision. They
call this unusual. I call it making the right call.
If Iowa's congressional delegation wants a waiver, then repeal the entire damned
law.
Otherwise, follow the law.
But that does not mean Trump is not waiving parts of Obamacare.
The New York Times reported:
Funny thing about presidential power. It belongs to all
presidents, not just the Marxist ones.
Some western nations, such as Sweden, are now adopting dietary
guidelines that encourage foods high in fat but low in carbs.
Cardiologist Aseem Malhotra, Croydon University Hospital in
London, says almost four decades of advice to cut back on saturated fats found
in cream, butter and less lean meat has "paradoxically increased our
cardiovascular risks." He leads a debate in the British Medical Journal
website that challenges the demonization of saturated fat.
A landmark study in the 1970s concluded there was a link between
heart disease and blood cholesterol, which correlated with the calories provided
by saturated fat. "But correlation is not causation," said Dr. Malhotra.
Recent studies fail to show a link between saturated fat intake
and risk of cardiovascular disease, with saturated fat actually found to be
protective, he said.
One of the earliest obesity experiments, published in the Lancet in 1956,
comparing groups on diets of 90 per cent fat versus 90 per cent protein versus
90 per cent carbohydrate revealed the greatest weight loss was among those
eating the most fat.
Professor David Haslam, of the National Obesity Forum, said: "The assumption
has been made that increased fat in the bloodstream is caused by increased
saturated fat in the diet … modern scientific evidence is proving that refined
carbohydrates and sugar in particular are actually the culprits."
Dr Malhotra said obesity has "rocketed" in the US despite a big drop in
calories consumed from fat. "One reason’ he said ‘when you take the fat out, the
food tastes worse." The confusion has led to people being 'over-medicated'
with statin drugs, such as Rosuvastatin
But why has there been no demonstrable effect on heart disease trends when
eight million Britons are being prescribed cholesterol-lowering drugs, he asked.
Adopting a Mediterranean diet after a heart attack is almost three times as
powerful in reducing death rates as taking a statin, which have been linked to
unacceptable side effects in real-world use, he added.
"It is time to bust the myth of the role of saturated in heart disease and
wind back the harms of dietary advice that has contributed to obesity."
Dr Malcolm Kendrick, a GP and author of The Great Cholesterol Con, "Around
the world, the tide is turning, and science is overturning anti-fat dogma.
Recently, the Swedish Council on Health Technology assessment has admitted that
a high fat diet improves blood sugar levels, reduces triglycerides improves
‘good’ cholesterol - all signs of insulin resistance, the underlying cause of
diabetes - and has nothing but beneficial effects, including assisting in weight
loss.
Professor Robert Lustig, Paediatric Endocrinologist, University of San
Francisco said ‘Food should confer wellness, not illness. And real food does
just that, including saturated fat. "But when saturated fat got mixed up with
the high sugar added to processed food in the second half of the 20th century,
it got a bad name. Which is worse, the saturated fat or the added sugar? The
American Heart Association has weighed in - the sugar many times over. Instead
of lowering serum cholesterol with statins, which is dubious at best, how about
serving up some real food?"
Timothy Noakes, Professor of Exercise and Sports Science, University of Cape
Town, South Africa said "Focusing on an elevated blood cholesterol concentration
as the exclusive cause of coronary heart disease is unquestionably the worst
medical error of our time. After reviewing all the scientific evidence I draw
just one conclusion - Never prescribe a statin drug for a loved one."
 Last week they announced
the results of the second year of the Oregon experiment, asking the important
question: what difference does Medicaid make? The answer, as Megan McArdle
reports, is not much, at least not in measurable health outcomes.
Last week they announced
the results of the second year of the Oregon experiment, asking the important
question: what difference does Medicaid make? The answer, as Megan McArdle
reports, is not much, at least not in measurable health outcomes.
In this the Oregon experiment agrees with the experts. The RAND study done in
the 1970s and reported in the 1980s found that giving people health insurance
didn't make a difference to their health; it just increased their consumption of
health care. And that aligns with the experts cited by James C. Riley in Rising
Life Expectancy: A Global History. Health care (called bio-medicine) is just one
of six factors ("public health, medicine, wealth and income, nutrition,
behavior, and education") undergirding our healthy, wealthy way of life. You can
check out the details at my "Experts Agree on Healthcare" here.
But that Oregon result set me to thinking not just about government healthcare
but entitlements in general.
Isn't the whole point of entitlements that they don't really make much of a
difference? I mean that if, e.g., Medicaid doesn't make a difference, it really
doesn't matter, except the waste of money. Same with education. We know that the
education system stinks, but America still seems to rub along.
We know that when you go the full metal jacket on government, where government
runs everything as in the totalitarian Soviet Union or Maoist China, the result
is mass starvation, and worse.
On the other hand, if the government does nothing, what's the point of climbing
the greasy pole to political power?
The fundamental fact of political rule is that government is an armed minority
occupying a territory, and it must sustain itself with requisitions from the
people that live there. It can do this with terror, but it's usually easier and
better for all concerned if government courts the support of the people by
handing out free stuff to its supporters. See my "Government and the Technology
of Power."
The only question is: How? How does the ruling class keep its power and pay off
its supporters? Plan A, full socialism or communism, is a failure. But taxing
and regulating the economy and diverting monies through the government to your
supporters seems like a real winner, as long as you don't overdo it like Europe
right now and the U.S. real soon.
Here's how it works:
People like pensions. So the government taxes the workers and then nobly hands
out Social Security checks to a grateful multitude. What difference did it make?
Not much, other than taking money from A to give it to B.
Women like healthcare. So the government taxes the rich and hands out healthcare
to every woman that wants to beat breast cancer or needs to care for her mother.
Without government, she knows, she could never afford it. But what difference
did it make? Not much, except take money from A and give it to B and drown
everything in a tidal wave of rules.
Parents want to give their kids a start in life. What better than to send them
to government child custodial facilities five days a week for sixteen years so
that they aren't a bother to mommy's career, and so that they don't compete in
the job market for dad's job? What has the government done? Well it's taken
money from A and given it to an army of teachers and administrators. Education
is no more than a by-product of paying off the teachers.
Rich people want to help the poor. So why not "pay at the office" and let the
government make war on poverty? It only costs about $0.6 trillion a year. But
the government doesn't really do anything about poverty except take money from A
and give it to B.
The key rule for a successful ruling class it this. Don't try to do anything or
make anything. Just talk about taxing the rich and the corporations and hand out
the free stuff.
But in real life the ruling class can't keep its mitts off. Rulers are fighters;
they want to direct the fight against evil; Democratic rulers fight poverty and
evil corporations. So Democrats can't resist the temptation to take over the
schools and form the minds of children themselves. They decide that an elite
corps of policy analysts and design and build a system to expand health
insurance to the uninsured and "bend the cost curve" at the same time.
Then all of a sudden government actually does start to make a difference and
things fall apart.
Because the only thing that political rulers can really do well without screwing
up is handing out free stuff to their supporters.
That's all political leaders have known how to do since the dawn of time.
Christopher Chantrill (mailto:chrischantrill@gmail.com) is a frequent
contributor to American Thinker. See his usgovernmentspending.com and also
usgovernmentdebt.us. At americanmanifesto.org he is blogging and writing An
American Manifesto: Life After Liberalism. Get his Road to the Middle Class.
Page reprinted from the American Thinker:
http://www.americanthinker.com/articles/../2013/05/entitlements_what_difference_does_it_make.html
Return to Index
MARCH
2013
SCHOOLBOY INVENTS EARLY CANCER
TEST
In the January 29,
2013 edition of Mail Online (www.dailymail.co.uk) Damien Gayle reported
on a new, low-cost test that can detect the early stages of pancreatic cancer.
Jack Andraka, a 15-year-old schoolboy from Crownsville, Maryland,
developed a simple dip-stick test for levels of mesothelin, a biomarker for
early stage pancreatic cancer found in blood and urine. In December of
2012 he was awarded the grand prize of $75,000 in scholarship funds at the 2012
Intel Science Fair. His test is 28 times faster, 28 times less expensive
and 100 times more sensitive than current tests. It could potentially
dramatically raise survival rates.
The test works in a similar way to diabetic testing strips, with
his paper strips using only a drop of blood to determine whether patients carry
the mesothelin biomarker. It is over 90% accurate and costs 3 cents and
takes 5 minutes to run. The sensor costs $3 and 10 tests can be performed
per strip. It has potential for applicability to other diseases, such as
tuberculosis, HIV, E Coli and salmonella.
He came up with the idea after reading an article about carbon
nanotubes. He was rejected by 197 scientists he solicited for help with
his research, some saying his idea simply would not work. Finally, Dr.
Anirban Maitra, a professor of pathology and oncology at Johns Hopkins
University agreed to give him space in the lab and mentored him through the
process of developing the test, which is in the process of being patented.
Jack plans to mass-market the tests and make them widely available
to the public. "Essentially what I'm envisioning here is that this could
be on your shelf at your Walgreen's, your K-Mart," he said. "Let's say
you suspect you have a condition. . .you buy the test for that. And you
can see immediately if you have it. Instead of your doctor being the
doctor, you're the doctor."
Return to Index
MAY 2012
FAT GENE PROTECTS AGAINST
DIABETES
In the April 2, 2012
edition of Express.co.uk, Jo Wiley reported on findings of a recent study
appearing in the online version of the journal Nature.
The study by researchers from Harvard Medical School in Boston,
Massachusetts have shown that the gene called ChREBP found in body fat can
actually prompt the body to resist diabetes by converting glucose sugar into
fatty acids. It also boosts sensitivity to insulin, the vital hormone that
regulates blood sugar.
Lead investigator, Dr. Mark Herman, said: "the general concept of
fat as all bad is not true. Obesity is commonly associated with metabolic
dysfunction that puts people at higher risk for diabetes, stroke and heart
disease, but there is a large percentage of obese people who are metabolically
healthy.
"We started with a mouse model that disassociates obesity from its
adverse effects."
Dr. Herman's team tweaked a "glucose transporter" gene in obese
mice that serves as a gateway for sugar. Usually, its activity in fat
cells drops with obesity.
The scientists found that when they increased glucose transporter
levels in obese mice -- allowing more sugar into their fat cells -- they were
protected against diabetes. Conversely, normal weight mice missing the
glucose transporter gene developed diabetes symptoms. Eight years ago
scientists learned that when fat cells start to have trouble taking in sugar, it
can be an early indicator of diabetes.
In healthy people, fat cells normally take up around 10% of the
sugars derived from food.
The researchers wrote: "These data suggest that selective
activation of adipose tissue ChREBP could be an effective therapeutic strategy
for preventing and treating type 2 diabetes and obesity-related metabolic
diseases."
Return to Index
JANUARY
2012
MEDICAL FREEDOM ZONES
By Jack McHugh, Dec. 6, 2011, Michigan Capitol Confidential
America’s health care system is
a dysfunctional mess for a fundamental reason: There is no real market in health
care. It was wrecked by a combination of incentive-skewing federal tax policies,
innovation-killing “fee for service” payment systems in the two federal programs
that pay for practically half of all health care consumed (Medicare and
Medicaid), restrictive state policies that create limited cartels of health care
professionals and facilities (reducing supply and so increasing price), and
more.
It all seems a hopeless quagmire, in part because instead of going to the
root cause of the dysfunctions to find solutions, politicians have instead
“doubled down” on market-killing policies, most recently with the monumentally
destructive Obamacare law, which comes on top of innumerable other
counter-productive government intrusions enacted on a bipartisan basis at both
the state and federal levels.
An interesting proposal from a Mackinac Center sister-think tank in Wyoming
seeks to cut this Gordian knot of perverse incentives and pernicious
restrictions with something called “medical freedom zones”: a “legally
recognized geographic area where health care professionals may provide services
and conduct research governed by professional associations and private
contracts.”
Here’s more from the paper on the idea authored by the Wyoming Liberty Group:
Both the federal and state governments hamper doctors’ ability to innovate
in medicine and to offer more affordable or alternative care. While the
federal government delays innovative medicine, state governments make
affordable care more difficult by limiting the number of doctors and saddling
those who do practice with difficult liability rules. Similarly, the ability
of care providers and patients to fashion their own agreements governing
medical procedures is entirely hamstrung through state regulation. The result?
More than 500,000 Americans fled the United States in 2008 for medical
tourism. The time for innovative reform is now.
Alas, even this creative solution cannot get to the root of the problem,
because the “freedom zones” don’t fix the two “original sins” primarily
responsible for wrecking health care, and which can only be fixed in
Washington: Allowing unlimited employer tax deductions for the cost of
employee health insurance, and Medicare and Medicaid’s “fee for service”
payment model.
The first of these, the tax code, is responsible for the third-party payment
system under which, unlike areas where markets truly exist, consumers don’t
behave like frugal, prudent value seekers, and providers aren’t forced by
competition to respond by becoming innovative, efficiency-generating value-maximizers.
The second source of the dysfunctions, Medicare and Medicaid’s payment system,
imposes price controls in a way that mostly takes away any reward for providers
reducing costs through innovation, destroying the incentive for them to even
try.
Fix those two things, and our health care delivery system can finally begin
to heal itself by becoming a real market. Leave them untouched, or worse yet
pile a huge new layer of regulation, subsidy and rationing on top of them (Obamacare),
and no fundamental improvement can ever be expected to occur in our health care
system.
It’s in our hands to make this right — but this requires forcing the
politicians in Washington to undo these core sources of dysfunction. If they
did, medical freedom zones could have the potential to accelerate the healing
process for our health care system.
Permission to reprint in whole or in part is hereby granted, provided that
the author and the Mackinac Center are properly cited.
http://www.michigancapitolconfidential.com
Return to Index
MAY
2011
LOW-FAT FOODS CAN BE BAD FOR
YOU
A report in the
April 11, 2011 edition of the Daily Mail Online (UK) says a study
performed at the Cambridge Nutrition Clinic shows that low-fat diets can
actually increase the risk of heart disease.
According to Nutritionist Dr. Natasha Campbell-McBride, a lack
of fats and cholesterol can damage the arteries and veins and lead to heart
attacks, strokes or organ failure because low-fat diets weaken the immune
system. She said: "The whole notion of saturated fat as some kind of bete
noire is simply wrong, as is the existence of so-called 'bad' cholesterol.
Fats and cholesterol help create and protect the white blood cells and millions
of other cells that repair the wall linings when damaged. The so-called
'bad' type of cholesterol, LDL, is specifically sent to the wound by the liver
and this is why patients with heart disease are seen to have high levels in
their body. Unfortunately, because LDL is found at the 'crime scene,' the
cholesterol is mistakenly blamed for the heart condition when in fact it is
nature's way of trying to combat it.
"We've been subjected to relentless medical advice demonizing
natural fats and cholesterol but they are in fact essential to life.
Extensive reviews of the available studies have shown me that the myth of heart
disease being due to fat is wrong. If the anti-fat message was correct
then we should by now be seeing a reduction in the level of heart disease when
in reality we're not."
People who follow low-fat diets do not have sufficient fats and
cholesterol to repair arteries, leading to scarring and narrowing of the
arteries and increasing the risk of dangerous blockages, which in turn increases
the chances of heart conditions and can also lead to degenerative diseases such
as Parkinson's and Alzheimer's.
Dr. Campbell-McBride's research is supported by American
scientists who found that strict vegetarians are at a 'substantial risk of
heart disease. She supports a balanced diet, which incorporates fat and
LDL cholesterol.
She added: "Heart disease is now the number one killer in
the UK despite a concerted effort by doctors and the NHS to improve the public's
cardiovascular health. It's now time to re-examine things and at the
center of that must be the foods we eat. By doing this, we can better
protect our bodies and help the horrific situation we are faced with today.
This mistaken view has only been around for 50 or so years while humans have
prized fat as the most valuable and nutritious food for millennia."
Dr. Campbell-McBride has released her findings in a new book
"Put Your Heart in Your Mouth."
Return to Index
FEBRUARY 2011
ANOTHER STATIN STUDY
DISCLOSES LIMITED BENEFIT
On December 19, 2011, The
Telegraph from London, reported on the latest study of statins which
suggested that for 3/4 of those taking them, they offer little or no value,
while exposing millions to the hazard of undesirable side effects.
The story of their
popularity began in 1975, when Henry Gadsden, the chief executive of Merck,
decided that he wanted to sell to everyone, rather than just people who were
ill. Thus began the arrival of "cholesterol consciousness": the thesis
that those indulging in (for example) bacon and eggs for breakfast boosted the
cholesterol level in the blood, causing the arteries to become narrow, and
making a heart attack more likely. While there may be some merit in the small
proportion of the population with a genetic predisposition towards high
cholesterol levels switching to a healthy diet, it did not lower the risk of
circulatory disorders. This led to the idea that cholesterol-lowering
drugs might be the answer.
The first statin,
Lovastatin, was launched in America in 1987, accompanied by an education program
encouraging everyone to get their cholesterol check and take medication if it
was found to be raised. Other drug companies got in on the act and from $3
billion in sales in the mid-1990s. Today it is a $26 billion business.
Guidelines were
established for cholesterol levels, and have forced the "normal" level ever
lower, making more people eligible for treatment.
The bottom line is that
statins are not nearly as effective in preventing heart disease and strokes as
they are portrayed. This applies to the vast majority of users whose
cholesterol level is deemed "high" but who are otherwise healthy. For
those people statins have no effect on mortality either way. In contrast,
for men -- but not women -- under 70 with a history of heart problems, they do
save lives.
Return to Index
AUGUST
2010
CHOLESTEROL STUDY
RAISES NEW CONCERNS
About 2 years ago, a study known as
the JUPITER (Justification for the Use of Statins in Primary Prevention) trial
raised the possibility of using cholesterol-busting statins to stave off
heart-related death in many more than just those with high cholesterol,
according to Charles Bankhead, ABC News MedPage Today staff writer on
June 29, 2010.
A second look by
researchers found that the results of the study are flawed and do not support
the benefits initially reported, showing no evidence of "striking decrease in
coronary heart disease [CHD] complications" and that the data set appears
biased.
This new look by Dr.
Michel de Lorgeril of Joseph Fourier University and the National Center of
Scientific Research in Grenoble, France and coauthors was reported in the June
28 issue of Archives of Internal Medicine.
While the original
supporters of the claim argue with this study, the French group points out that
9 of the 14 authors of the study have financial relationships with AstraZeneca,
which sponsored the trial.
Authors of another article
in the same issue of Archives reported that a review of 11 primary-prevention
trials showed no effect of statin therapy on deaths in high-risk patients.
On the basis of their
review, do Lorgeril and coauthors concluded that " time has come for a critical
reappraisal of cholesterol-lowering and statin treatments for the prevention of
CHD complications. The emphasis on pharmaceuticals for the
prevention of CHD diverts individual and public health attention away from the
proven efficacy of adopting healthy lifestyle, including regular physical
activity, not smoking, and a Mediterranean-style diet."
In another analysis
reported in the same issue of the journal, Dr. Kausik K. Ray of the University
of Cambridge in England examined the findings of 11 randomized clinical trials
involving a total of 65,229 patients to see if statins cut death rates among
intermediate and high-risk people with no history of cardiovascular disease.
In this study, too, the support for statin use was lacking.
In an editorial that
accompanied the two articles, Dr. Lee Green of the University of Michigan in Ann
Arbor said the de Lorgeril and Ray studies add fuel to a high-stakes debate.
"In the long term,
although sincere advocates on both sides will try to convince us otherwise we
really must admit that we do not know," Green Wrote. "We need good
research to find out, and, as de Lorgeril and colleagues point out, that search
must be free of incentives to find any particular desired answer."
Return to Index
FEBRUARY 2010
THE
TRUTH ABOUT OBAMACARE
By John Lilly, January 13, 2010
A senior Obama Administration
official almost let the cat out of the bag about the real impact of Obama-style
health care "reform." Here's the background.
The three most
important things in real estate are location, location, and location. In health
care, one could argue that it's reimbursements, reimbursements, and
reimbursements. One in every six workers receives a paycheck that depends on
physician and hospital reimbursement for services. Except for Medicaid, Medicare
reimbursement rates are the lowest of all entities that reimburse physicians and
hospitals. All private insurance and Medicare Advantage reimbursements are
higher than traditional Medicare ones. Medicare and Medicare Advantage plans
take a $425-billion cut in the current health care reform legislation.
In 2008, a Physician
Foundation survey found that 36% of physicians said Medicare reimbursement is
less than their cost of providing care, and 65% of physicians said that Medicaid
reimbursement is less than their cost of providing care. Raise your hand if you
work for free. Then why is the administration asking one-sixth of all U.S.
workers to do just that?
Larry Summers, the
Obama administration's Director of the National Economic Council, spoke at The
Economic Club of Washington at their April 2009 meeting. C-SPAN was there, and
at roughly minute 41, Summers said the following:
That's why health
care reform is so important because a large fraction of the federal budget is
health care and if health care spending is growing three to four percent a
year faster than the rest of the economy then there is no way that the federal
budget can be under control. And if you try to control federal spending
without controlling overall health spending you know what's going to happen.
The people in the federal programs aren't going to be able to ...
Then he paused before
continuing:
The health care
system isn't going to want to serve the people in the federal programs. That's
why the health care agenda is crucial to the long term financial
sustainability agenda.
I think it is obvious
that Summers was going to say that "the people in the federal programs aren't
going to be able to find a doctor if you have Medicare," but he rephrased it
before his original thought came out of his mouth. When he talks about overall
health spending, he is including all public and private entities that reimburse
physicians and hospitals. Federal spending includes just Medicare and Medicaid.
When Medicare
reimbursement does not cover the cost of doing business, guess who will have a
tough time finding a doctor. If there is a choice, then doctors, like any
rational consumer, will prefer plans like Medicare Advantage and private
insurance, which have higher reimbursement rates. The administration's idea of
holding down costs is forcing all reimbursements down to Medicare levels or
lower. They know that if there are alternatives, patients who are stuck with
traditional Medicare won't be able to find a doctor. Recently, one of the Mayo
Clinics in Arizona stopped taking Medicare because it's a money-loser. Mayo's
hospital and four clinics in Arizona, including the one that stopped taking
Medicare, lost $120 million on Medicare patients last year. The program's
payments covered only 50% of the cost of treating elderly primary-care patients.
If all reimbursement
rates are forced down to Medicare rates or lower, then get ready for five-minute
doctor visits and waiting times measured in weeks and months before appointments
for major diagnostic testing like MRIs.
Unfortunately, the
Republicans do not have the answers, either. Their proposals will not control
costs. Only when you introduce free-market competition and eliminate the current
reimbursement system will you get lower costs. That will require a fundamental
change in Medicare and all reimbursement systems.
John Lilly, MBA, D.O.
is a family physician and the vice president of The YOUNG Conservatives of
America (tycoa.com).
Page Reprinted by
permission from the American Thinker: http://www.americanthinker.com/2010/01/the_truth_about_obamacare.html
Return to Index
OCTOBER 2009
STORIES FROM ENGLAND
ON NHS
In articles recently published in
England on the National Health Service (NHS), their socialized medical care,
there is one horror story after another. Remember, England is a country of
about 60 million people with the NHS being the largest employer in the country
-- over 1.5 million. Only the Chinese Army and Walmart have more
employees. Consider the size of the program for over 300 million
Americans, and whether or not the government could possibly manage a program
that size any better. . . .
On Sep. 4, 2009, the
Mail Online, reported that the number of medication errors have doubled in
two years. While the reported number of more than 86,000 mistakes,
including drugs being given to the wrong person or the wrong dose were
endangering patient safety. However, it is believed that fewer than 10% of
errors were being reported to the NHS, meaning the true number was probably
close to one million.
On Sep. 8, 2009, the
MailOnline reported that thousands of women are being denied better
osteoporosis drugs because of unnecessarily restrictive Government guidelines
established by the drug rationing body, the National Institute for Health and
Clinical Excellence (NICE). This is the group that was patterned in the
Stimulus Bill and is already established in law. (This is why Obama says
they don't need to put the panel in the proposed health care/insurance/single
payer plan now under consideration. It is already established.)
On Sep. 9, 2009, the
guardian.co.uk reported that the Conservative party says hospitals are at a
breaking point and claims that a second wave of swine flu could result in a bed
shortage.
However, this shouldn't
have been a surprise. On Aug. 26, 2009, MailOnline reported that
shortages of hospital beds and midwives forced 4,000 mothers to give birth in
elevators, offices, corridors and hospital toilets.
They appear to be the
lucky ones. The Telegraph.co.uk reported on Sep. 2, 2009 that a
group of experts who care for the terminally ill claim that some patients are
being wrongly judged as close to death. Under NHS guidance introduced
across England to help doctors and medical staff deal with dying patients, they
can then have fluid and drugs withdrawn and many are put on continuous sedation
until they pass away.
The Telegraph.co.uk
reported on a particular case on Sep. 8, 2009. The daughters of a
stroke victim claimed that her father was wrongly placed on an NHS scheme for
the terminally ill which was causing him to die too soon. Once the removal
of fluids, medication and other treatments has started, the patient weakens and
there is no going back. The daughters believe that the hospital personnel
decided from the beginning that he was 95 so should be written off.
On Sep. 15, 2009, the
MailOnline reported that more than a quarter of families are not told
when life support is withdrawn from terminally-ill loved ones, leading to a fear
of "backdoor euthanasia" especially for patients whose average age was 81.
The decision not to
treat is not limited to old people. On Sep. 9, 2009, the MailOnline
reported on a woman who was told that it was against the rules to treat or try
to save her premature baby. He was born 2 days prior to 22 weeks. He
lived for almost 2 hours without any medical support, breathing unaided, had a
strong heartbeat, and was moving his arms and legs. However, medics
refused to admit him to a special care baby unit.
When the government
"pays" it sets the rules. If these aren't death panels, I don't know what
they would look like.
Remember, when our
country was established, the Constitution established the federal government
with limited power. The representatives were supposed to work for the
people. Every day, we are getting closer to working for the government.
We are on the way to being subjects, not citizens.
Return to Index
AUGUST
2009
CANADA'S NATIONAL
HEALTH CARE AND BABIES
Investor's Business Daily, on
June 30, 2009, noted that under Canada's National Health Care System, fragile
babies depend on the United States in many cases. Under the government
planned system used there, neonatal care is simply not available in many cases
and has to be obtained from American hospitals across the border.
Infant mortality rates
are often cited as a reason socialized medicine and a single-payer system is
supposed to be better than what we have here. But, according to Dr. Linda
Halderman, a policy adviser in the California State Senate, these comparisons
are bogus.
As she points out, in
the US, low birth-weight babies are still babies. In Canada, Germany and
Austria, a premature baby weighing less than 500 grams is not considered a
living child and is not counted in such statistics. They're considered
"unsalvageable" and therefore never alive.
Norway boasts one of
the lowest infant mortality rates in the world -- until you factor in weight at
birth, and then its rate is no better than in the US.
In many countries
babies that survive less than 24 hours are considered stillborn or a
miscarriage. In some, a baby must be 30 centimeters long to be considered
a live birth.
In 2007, there were at
least 40 mothers and their babies who were airlifted from British Columbia alone
to the US because Canadian hospitals didn't have room. Since 2000, 42 of
the world's 52 surviving babies weighing less than 400 grams (.9 pounds) were
born in the US.
Return to Index
MARCH
2009
SURPRISES IN THE "STIMULUS"
BILL
 David Limbaugh in
his Feb. 20, 2009, column on Townhall.com noted how the Democrats have
been diminishing the freedoms and rights of Americans since Obama was elected.
In doing so, he brought up the gigantic "Stimulus" bill which had to be passed
before anyone could read it.
David Limbaugh in
his Feb. 20, 2009, column on Townhall.com noted how the Democrats have
been diminishing the freedoms and rights of Americans since Obama was elected.
In doing so, he brought up the gigantic "Stimulus" bill which had to be passed
before anyone could read it.
Former New York Lt. Gov. Betsy McCaughey, at the personal expense of
incurring the fury of such liberal mouth foamers as MSNBC's Keith Olbermann,
has helped expose hidden health care provisions in President Obama's stimulus
nightmare that "will affect 'every individual in the United States.'"
The bill creates a new bureaucracy, the Office of the National Coordinator
for Health Information Technology, which "will monitor treatments to make sure
your doctor is doing what the federal government deems appropriate and cost
effective." Note: not what your doctor deems appropriate, but what the federal
government does. Doctors and hospitals will face penalties if they fail to
kowtow to this fiat requiring uniformity. This new bureaucracy will receive
greater funding than "the Army, Navy, Marines, and Air Force combined."
Worse, the bill will result in the rationing of care for the elderly. But
that's OK because Big Brother has determined that individuals will benefit in
their younger years and will have to sacrifice later. I'm not making this up.
This is one of the rationales defenders of these innovations are serving up.
Much of the impetus for these health care changes came from disgraced
former Sen. Tom Daschle, who would be head of Health and Human Services right
now but for his little tax issue. McCaughey shares revealing gems from
Daschle's 2008 book, "Critical: What We Can Do About the Health-Care Crisis."
Among them are his opinions that doctors must give up autonomy and "learn to
operate less like solo practitioners" and that seniors will have to learn to
deal with -- rather than receive treatment for -- conditions that arise from
their age.
Perhaps the most chilling aspect of this particularly noxious stealth
provision of the stimulus scheme is not what's in it, but how it -- and other
such free market-destroying provisions -- were rushed through under deliberate
cover of darkness. McCaughey attributes this strategy to Daschle, as well.
A year ago, McCaughey tells us, Daschle warned that the next president
should not make the same mistake the Clintons made with Hillary Care, which
was to allow debate. Daschle wrote: "If that means attaching a health-care
plan to the federal budget, so be it. The issue is too important to be stalled
by Senate protocol."
So much for "liberal" democracy. So much for transparency. So much for a
new era of hope and change.
If Obama's plot to micromanage health care from on high doesn't move you,
how about the abolition of welfare reform provisions imbedded in the bill?
Never mind that welfare reform has been such a smashing success that even Bill
Clinton tries to take credit for it despite his twice-frustrated efforts to
block it. What's important is not whether it has worked, but whether it
satisfies Obama's vision for expanding the welfare state.
You have to keep your eyes open with this bunch.
The only way to stop this nonsense is to get Congress to pass another bill
overturning these changes. Contact Rep. Bart Stupak at
http://www.house.gov/stupak
and Sens. Carl Levin at
http://levin.senate.gov/contact/index.cfm and Debbie Stabenow at
http://stabenow.senate.gov/email.cfm.
If you wish to phone them, call the Congressional Switchboard -- 1-202-224-3121
Return to Index
FEBRUARY
2009
MORE
TO THINK ABOUT WITH HEALTHCARE
The Democrat administration is
working hard to try to impose government controlled healthcare on the American
people.
The Wall Street
Journal noted on Jan. 21, 2009 that the US House of Representatives passed a
major expansion of the State Children's Health Insurance Program. The
program will more than double in size with $73.3 billion in new spending over
the next decade (less than the true cost because of an accounting gimmick).
This program, which was supposed to help children from working poor families
will now cover everyone up to 300% of the federal poverty level -- $63,081 for a
family of four. According to the Census Bureau the US median income is
$50,233. States can get a waiver to go even higher.
Every time the program
grows, it displaces private insurance. National taxpayers end up paying 65
to 83% of the total cost. When states make health-care promises they can't
afford -- such a New York, which expanded the program to 400% of poverty -- the
feds always step in with a bailout. This is all supposed to be paid for
with an increase in the federal tobacco tax from 39 cents to $1 a pack,
financing a permanent and growing entitlement with a declining corps of smokers.
Dr. Scott Gottlieb, a
resident fellow at the American Enterprise Institute in an article in The Wall Street Journal
on
Jan. 20, 2009 noted that in Britain, a government agency evaluates new medical
products for their "cost effectiveness" before citizens can get access to them.
The agency has concluded that $45,000 is the most worth paying for products that
extend a person's life by one "quality-adjusted" year. (By their
calculus, a year combating cancer is worth less than a year in perfect health.)
As a part of the
$800-plus billion stimulus package, studies will compare different drugs and
devices to "save money and lives" are included. Incoming Secretary of
Health, Tom Daschle, has long advocated a US approach based on the British
model, arguing that the only way to reduce spending is by allocated medical
products based on "cost effectiveness."
Many if Britain object
to the constraints which deny cancer patients many effective new drugs that are
widely prescribed in the US. Of course, the rich are able to opt out of
the British controls, but the politicians control access for most people.
In the
irishtimes.com on Jan. 19, 2009, noted that with the Irish national health
service, three-quarters of a million people with a neurological condition
are waiting 18 months to see a consultant and 10 months to have an MRI scan in
order to secure a diagnosis, is now the norm.
ABC News, in an
article by Dr. Paul Hsieh, on Jan. 11, 2009, noted that in Japan, the government
regularly checks the waistlines of citizens over age 40. Anyone who is deemed
too fat is required to undergo diet counseling, "reeducation" if that doesn't
work and stiff fines. The government argues that it must regulate
citizens' lifestyles because it is paying their health costs.
The British government
has banned some television ads for eggs on the grounds that they were promoting
an unhealthy lifestyle.
New Zealand banned the
entry of persons whose obesity would "impose significant costs . . . on New
Zealand's health or special education services."
Hsieh noted that nanny
state regulations have exploded here in the US as well -- everything from
smoking, banning trans fats, and prohibiting new fast food restaurant in South
Los Angeles, California. These, and other proposals to tax certain foods
are certain to increase if government takes over and adopts universal health
care.
On Jan. 11, 2009, the
dcexaminer.com noted in an editorial that the much-touted Massachusetts
plan to force all residents to buy health insurance has turned out to be an
embarrassing flop.
Within a year after the
law passed, state insurers were already jacking up rates to twice the national
average. 43 mandatory benefits, including many that most people did not
need or want, such as invitro fertilization -- raised the costs as much as 56%.
Small businesses with
more than 10 employees were required to provide health insurance or pay an extra
fee to subsidize uninsured low-income residents, yet the overall costs of the
program increased more than $400 million, 85% higher than original projections.
To make up the difference, payments to health care providers were slashed, so
many doctors and dentists in Massachusetts began refusing to take on new
patients, leaving some people to wait over a year for a simple physical exam.
Naturally, the original
goal, to make certain everyone has coverage has not been met, despite the
disastrous cost increases.
Rushing forward to
implement universal socialist medical coverage would be a major mistake.
Return to Index
JANUARY
2009
WELCOME TO ACORN GENERAL
HOSPITAL
By Carol Peracchio, December 15, 2008
I've been a registered nurse
for 30 years, so the future of American health care is one of my greatest
concerns. Now that Mr. Obama has won the election, I decided to investigate what
may be facing patients and health care workers.
I started my research at Barack Obama's website and his Plan for a Healthy
America. What a waste of time. It read like a treatise from a beauty pageant
contestant.
What kind of medical expertise does Barack have? Remember th[e] youtube
where his teleprompter malfunctioned? He stumbled through an excruciatingly
inept explanation of how health care costs can be lowered if kids with asthma
could just be provided "breathalyzers," or "inhalators" instead of cluttering up
emergency rooms.
This brilliant (as we're told ad nauseam) Ivy League lawyer-savant wants
to run our health care but apparently is ignorant of the word inhaler. (There
must have been more than one nurse in that crowd shaking her head and thinking,
"Great. Another dunce.")
Certainly Obama is not the first politician who clumsily attempts to feign
a molecule of medical knowledge in order to sway voters who know even less.
Obviously, he is not capable of writing (or possibly even reading) any health
care legislation. I decided I'd need to find out the views of his advisors.
Since his wife Michelle had actually worked for a hospital, I began with her.
Let's start with her resume. Michelle came to the University of Chicago
Medical Center from The University of Chicago, where she ran something called
the University of Chicago Community Service Center:
which offered new opportunities to student, staff, and faculty for
service learning, volunteerism and civic engagement. This was a first step for
the University to engage students in community service activities.
Looks like Community Organizing was an Obama family affair!
In 2002 Michelle was recruited by the Medical Center, where she first was
hired as the Executive Director of Community Affairs. After three years, she was
promoted to Vice President for Community and External Relations and her salary
was tripled to over $300,000.00 a year. It is entirely coincidental, we are
assured, that her husband was elected to the US Senate the year of her
promotion.
When she was promoted, Michelle said:
My goal in this position is to continue to broaden the Hospitals'
relationships with our neighborhood and with our city. We have an obligation
to ensure that we use our resources on behalf of our neighborhood and our
city. In this new role, my goal is to better integrate community engagement
into the culture of this institution and to expand our partnerships with local
organizations and institutions.
Nowhere in this mishmash of goalspeak is there any hint of taking care of
sick people. It looks like Michelle's view is that the hospital has "an
obligation to ensure we use our resources on behalf of our neighborhood and our
city." Community organizing meets health care.
And what did Michelle accomplish as a hospital Vice President? According to her
resume:
She grew a staff of two into a diverse, 23-person team that carries out
a threefold mission of improving community-based health care, increasing
business opportunity of South Side businesses and enhancing the Medical
Center's considerable service to the surrounding community.
So her first accomplishment was increasing the size of her own department
eleven-fold! Forget the use of the word "diverse". The sheer amount of
expenditure involved in a 23 person department with a Director earning over 300K
is breathtaking! I can just imagine the response to clinical department heads
submitting budget requests in the Era of Michelle: "Sorry, there's no money for
(write your request here). Vice Presidents married to US Senators don't come
cheap!"
Michelle declared she had a threefold mission for her position at the
hospital. First, "improving community-based health care." At least this claim
involves health care. However, I doubt it took a very expensive Senator's wife
to do it. I've known social workers who accomplish this every day with much less
support and no fanfare.
Her second mission was "increasing business opportunity of South Side
businesses."
Increasing business opportunity? Call me crazy, but for 30 years I've been
under the impression that hospitals exist to take care of sick people. The
patient comes first! (At least that's what they always told us during those
interminable new employee orientation days.) Sometimes the hospital hires area
businesses in order to improve the delivery of care. But the businesses aren't
the focus. The patient is.
Next, Michelle enhanced "the Medical Center's considerable service to the
surrounding community." So how did Michelle enhance the hospital's community
service? Here's a partial list from her resume:
Service Learning Initiatives, Day of Service and Reflection,
Adopt-A-School programs, Principal for a Day and Real Men Cook celebrations.
Sounds like a $300,000.00 agenda to me! Seriously, most of these
"accomplishments" sound exactly like the Eagle Scout projects completed by my
son's Boy Scout Troop! The difference being my son and his friends didn't charge
the local hospital.
For all the glowing praise heaped upon Michelle for her External Relations
work, I can see that she did seem to have one problem. Her day of Service and
Reflection drew less than 300 volunteers. (I'm sure that's including the diverse
staff of 23). Out of a workforce of 9,500 Medical Center employees, this is a
dismal turnout.
But it's predictable when a country has a free market health care system.
It works like this: The nurse goes to the hospital that hires her for, let's
say, 1/6th the pay of an External Relations Director. The nurse agrees to
practice nursing for 40 hours a week, more if the floor is short-staffed. At the
end of her 8 or 12-hour day the nurse goes home.
The last thing 9,200 Medical Center employees want to do after a tough
week is to spend a day "reflecting" with Michelle and her diverse staff. And
because, at the moment, the nurse works for the hospital and not for Barack's
federal government, she has the freedom to say "No thanks."
But this free market setup was all wrong for Michelle's goal: to mine the
rich resources of money and hospital personnel for the necessary work of
community organizing. The money wasn't too difficult -- just divert those
resources that have been set aside for raises, or equipment, or education. Then
tell the staff how broke the hospital is because "reimbursements aren't keeping
up with expenditures."
The problem is that health care workers aren't college students. Forced
"service learning hours" aren't part of the job description, and if one hospital
tells me that taking part in Michelle's "Adopt-A-School" program is part of my
contract, I'll head over to the hospital down the road. And I'll deck the first
limousine liberal who tells me that health care workers need to be forced to
help their communities.
Drop by any health fair, Relay for Life, blood drive, or free clinic. All
staffed by volunteers, many of them health care workers. Think back to 9/11. I
knew of so many nurses, paramedics, and other health professionals who jumped in
their cars and just drove to New York and DC to serve.
But try to imagine health care in the world of Obama. All of us will be
enlisted in the Community Service army, where patient care is merely ancillary
to your job. Now we will leave work to go staff the after school program at the
new community center. Next weekend it's over to the mall where we will work the
voter registration table. It's all part of "enhancing the hospital service to
the community." Because in Barack and Michelle's world, there's no individual
patient. Only a vast, nebulous "community." Welcome to ACORN General.
Page reprinted by permission from The American Thinker: http://www.americanthinker.com/2008/12/welcome_to_acorn_general_hospi.html
Return to Index
DECEMBER 2008
THOSE
46 MILLION WE HEAR ABOUT
In the Nov. 21, 2008 edition of
The Wall Street Journal, William Snyder analyzed the alleged 46 million
uninsured to see if a total reorganization of the nation's health care system is
really warranted.
While many Americans
believe the uninsured are too poor to purchase coverage and government programs
are not available to them, that is not the case. A study published in
Health Affairs in November 2006 estimated that 25% were in fact eligible for
government coverage and another 20% could probably afford coverage on their own.
Applying those percentages to today's uninsured population leaves about 25
million people who need some assistance.
A study published by
the California HealthCare Foundation (CHCF) in April 2000 found 50% of
California residents at twice the poverty level had received care for which they
were charged, another 8% received care for which they were not charged. 89% of
them were very or somewhat satisfied with the care they received and only 15%
went to the emergency room as opposed to a doctor's office or clinic.
Another study, published by Health Affairs in August had similar findings, and
estimated that uninsured Americans will receive $86 billion worth of health care
in 2008.
The CHCF study found
that the 1.3 million uninsured who received care for which they were charged,
80% paid for it, and almost half the remaining 20% were paying in installments.
The Health Affairs study estimated that the uninsured would pay for $30 billion
of their health care costs this year out of pocket.
For the millions of the
uninsured, then, who are getting and paying for satisfactory care on their own,
foregoing needed care and sticking the public with huge ER bills is a myth.
These studies bring
into question the necessity for significant expansions of government programs,
legal requirements for everyone to carry insurance, or a combination of the two.
It would be better to encourage those who are currently eligible for government
programs to enroll and deal separately with that small number of persons who
truly have fallen through the cracks.
Return to Index
MAY
2008
MORE CHOLESTEROL NONSENSE
In the May,
2007 newsletter, the article “High Cholesterol Is Good for You” reported on the
British study that showed that statin drugs, such as Lipitor, Crestor and other
widely used brands, did not work for women and for very few men.
Now, there is a new study showing that Vytorin and Zetia failed to improved
heart disease even though they worked as intended to reduce three key risk
factors. These drugs have racked $5 billion in sales. The study was completed 2
years ago, but the results were just presented at a recent American College of
Cardiology conference in Chicago and published on the internet by the New
England Journal of Medicine, according to an Associated Press report of March
31, 2008.
While these drugs dramatically lowered LDL (bad cholesterol), fats in the blood
called triglycerides and a measure of artery inflammation, CRP, they showed NO
BENEFIT in reducing plaque build up in the arteries, which is thought to be a
way to reduce risks of heart disease.
The interesting thing to note, is that Yale Cardiologist Dr. Harlan Krumholz,
recommended that doctors and patients should return to statins. That is also an
interesting recommendation in view of the report published in Lancet (the
Medical Journal of England) and featured in our May 2007 report.
Return to Index
MARCH 2008
MEDICAL SURPRISES
The Australian
Broadcasting Corporation, on January 24, 2008, reported on a 15-year-old
Australian liver transplant patient who has made medical history.
Demi-Lee Brennan had a liver transplant after she suffered
liver failure. Nine months later, doctors at Sydney's Westmead Children's
Hospital were amazed to find the teenager's blood group had changed to the
donor's blood type. The stem cells from her donor had penetrated her bone
marrow. Her immune system had almost totally been replaced by that of the
donor, meaning she no longer had to take anti-rejection drugs.
Now, the medical team is trying to determine how the phenomenon
happened and whether it can be replicated. It is possible that the type of
liver failure she had, which required some drugs to suppress the immune system
and the fact that she suffered an infection with cytomegalovirus, which can also
suppress the immune system had a role to play.
If this can be replicated with other patients, transplant
patients may not have to take the anti-rejection drugs which have significant
side effects.
The case was published in the New England Journal of
Medicine.
The Daily Mail, from England, reported on Jan. 28, 2008,
about a school boy who was suddenly cured after 9 years of deafness.
It seems that Jerome Bartens, 11, was diagnosed as deaf in his
right ear when he was just 2. After years of treatment and difficulty in
school and in life because of his hearing problem, he was playing pool with
friends in a church hall when he felt a sudden pop. He put his finger in
his ear and there was the tip of a cotton wool bud which had been wedged there
for almost 10 years. He could hear immediately.
His family believes that he put the cotton bud in his ear as a
toddler and the cotton came off the plastic stem.
There is no explanation for why the many doctors who have
examined Jerome over the years failed to find the bud.
UPI reported on Jan. 17, 2008, that blood samples
revealed infection with a parasite carried by domestic animals may increase the
risk of schizophrenia, a study published in the American Journal of
Psychiatry found. Of 180 subjects diagnosed with schizophrenia, 7% had
been infected with toxoplasma prior to diagnosis, compared to 5% of the healthy
military recruits.
While this 24% difference in risk of developing schizophrenia
may seem small, it is important because of the possibility of treating patients
with anti-parasitic drugs may affect the progression of schizophrenia.
The parasite toxoplasma gondii can come from cat feces or
undercooked beef or pork. Infections rarely cause symptoms and the
parasite can lay dormant for years.
Return to Index
NOVEMBER 2007
THOSE AUSSIES ARE CREATIVE
On October 10,
2007, The Sydney Morning Herald reported on the case of a 24-year old
tourist who apparently tried to do himself harm swallowed ethylene glycol, an
ingredient in antifreeze, which is highly toxic.
The accepted treatment of this condition is to administer
pure alcohol, which the Australian doctors at Mckay Base Hospital in Queensland
did until they exhausted their supply.
Not be thwarted, they ordered a case of vodka and drip-fed
him the equivalent of about 3 standard drinks an hour for 3 days in the
intensive care unit.
One of his treating doctors, Todd Fraser said" "Fortunately
for him, he was in a medically induced coma for a good portion of that. By
the time he woke up, I think his hangover would have well and truly gone."
The Italian man, treated in August, made a successful
recovery and returned home.
Return to Index
OCTOBER 2007
MORE PROBLEMS WITH CANADIAN
HEALTH SERVICES
On September 18,
2007, Canada.com published an article by Pamela Cowan, Saskatchewan News Network
reporter, about a lady named Joyce Manz who has been on a wait list for back
surgery since August 2006. When she called the Saskatchewan Surgical Care
Network in September, she was told her surgery will not take place until
February. No reason was given.
She got a prescription for morphine last week to help control
the shooting pain in her right leg. She is afraid that by the time the surgery
takes place, she will be addicted to morphine.
Saskatchewan Health Minister Len Taylor acknowledged that
surgical waits are long in some areas, but said the situation is improving and
that since 2004, the Surgical Care Network’s figures show that the number of
patients waiting for surgery has declined by over 1,000. He did not say how many
people are waiting.
How long do you want to wait for “free” medical care?
Return to Index
SEPTEMBER 2007
MEDICAL DEVELOPMENTS
In the July 26,
2007 edition of CBC News, a report from the British medical journal,
Lancet, Dr. Stanley Zammit, one of the authors of the study published on
July 27, stated that smoking pot may increase the risk for the type of psychosis
commonly associated with schizophrenia. Occasional smokers were 40% more
likely to suffer from psychosis, while dedicated tokers who used marijauna daily
or weekly increased their risk by 50 to 200 per cent. The risk of
developing schizophrenia remains about 5 in 1000 people.
Zammit and his colleagues examined 35 studies that tracked tens
of thousand of people for periods ranging from one to 27 years to examine the
effect of marijauna on mental health. "The available evidence now suggests
that cannabis is not as harmless as many people think," said Dr. Zammit.
While there are questions about whether marijauna use increases
the risk of psychosis, or whether there is something about the users that causes
the psychosis is not clear.
Wende Wood, drug use and drug information pharmacist with the
Centre for Addiction and Mental Health in Toronto, Canada, agrees. She
says chronic pot use can push people predisposed to psychosis over the edge.
 Reuters
reported on August 1, 2007, about a study by Astrid Limb and her colleagues at
the University College London's Institute of Ophthalmology, in which they
studies the ability of zebrafish to regenerate damaged retinas.
Reuters
reported on August 1, 2007, about a study by Astrid Limb and her colleagues at
the University College London's Institute of Ophthalmology, in which they
studies the ability of zebrafish to regenerate damaged retinas.
The researchers said that they had successfully grown in the
laboratory a type of adult stem cell found in the eyes of both fish and mammals
that develops into neurons in the retina. They studied Mueller glial cells
in the eyes people aged from 18 months to 91 years and found they were able to
develop them into all types of neurons found in the retina and grow them easily
in the lab.
They hope to be able to inject a person's own stem cells into
his own eye and treat diseased retinas causing blindness, such as macular
degeneration, glaucoma and diabetes-related blindness.
On August 13, 2007, The Globe and Mail (Canada) reported
that a team of scientists at the British Columbia Cancer Agency discovered a
unique gene that can stop cancerous cells from multiplying into tumors.
The team, led by Dr. Poul Sorensen, says the gene, HACE 1, has
the power to suppress the growth of human tumors in multiple cancers, including
breast, lung and liver, particularly when it is kick-started.
The study appeared in Nature Medicine advance
online edition of the September 2007 issue.
Return to Index
AUGUST
2007
BONE MARROW TREATMENT
SUCCESSFUL
In the Feb. 12, 2007 edition of The Jerusalem Post,
Julie Siegel-Itzkovich, reported on a first-time procedure in Israel.
A woman suffering from secondary acute leukemia was saved by
umbilical cord blood donated by two mothers after they gave birth. One
cord does not contain enough blood for the procedure. Stem cells from cord
blood do not have to be the exact tissue type of the recipient, unlike bone
marrow from adults.
A spokesman for Sheba Hospital in Tel Hashomer, where the
procedure was performed, said the graft "took in 2 weeks rather than the month
it usually takes for bone marrow. Since only one in four patients who need
a bone marrow transfer are successful in finding a match, the cord blood
donation offers great potential in increasing the pool.
The establishment of cord blood banks makes it easier to find
suitable donors.
Previously, the hospital had transplanted stem cells from
umbilical cord blood only into children, one dose at a time. The use of
two doses at one time made the treatment faster and more effective. The
patient is now in good condition.
Return to Index
JULY
2007
SOCIALIZED MEDICINE =
RATIONING
In the June 26,
2007 edition of The Scotsman, Lyndsay Moss, Health Correspondent,
reported that the British Medical Association (BMA) held a conference in which
they were told that the government and National Health Service (NHS) must be
more open with patients about the need to ration treatments and services in a
system with a limited pot of cash.
Alex Smallwood, from the BMA's junior doctors committee said:
"It is no longer possible to provide all the latest to absolutely everybody
without notable detriment to others."
Reducing the choice of patients would require the drawing up
a list of acceptable treatments, but, might include a restriction on treating
things like hernias and varicose veins - conditions with which people could
live.
And, in Scotland, young doctors, who have been trained at a
cost of 250 pounds paid for by the taxpayers, are being forced to leave the
country. She and others who have trained to be General Practitioners have
no place to work. A few have been able to get jobs in England, but many
have been forced to go overseas for employment.
See how well everything works when the government runs it.
Return to Index
JUNE
2007
STAR TREK SCANNERS ON THE HORIZON?
In the May 22, 2007 edition of the
Telegraph.co.uk, was a report that scientists have moved closer to
developing a Star Trek-type scanner that can identify the molecular indications
of cancer and other diseases without surgery.
The discovery that x-ray images
contain patterns that can help doctors translate the genetic "language" of
tumors is being compared to the "Rosetta Stone" that enabled archeologists to
read hieroglyphics.
The research, reported in an online
edition of Nature Biotechnology, revealed previously missed patterns in
X-ray images from CT scans that correlate with genetic profiles, giving hope of
developing a "tricorder" type devise that appeared in almost every episode of
Star Trek. It was used to non-invasively scan matter to determine its
molecular makeup.
The object is to come up with a way
to systematically connect gene activity, obtained by "reading" DNA using devices
called microarrays, to imaging patterns to disease process. Radiologists,
already expert in recognizing the differences between normal images and those
reflecting changes caused by disease, could hold the key to the technology's
potential.
Return to Index
MAY 2007
HIGH CHOLESTEROL IS GOOD FOR
YOU
Most of you will
now think your editor has gone off the deep end, (which may be true) but, an article in the Daily
Mail, (UK) on Jan. 23, 2007 by Dr. Malcolm Kendrick, discussed an article in
the British medical journal The Lancet. Trying to lower your
cholesterol level by taking statin drugs is probably not worth it.
Women don't benefit from taking them at all, nor do men over
69 who haven't had a heart attack. There is a very faint benefit if you
are a younger man who also hasn't had a heart attack. Out of 50 men who
take the drug for 5 years, one will benefit.
What your doctor should be saying is the following:
A high diet, saturated or otherwise, does not affect blood
cholesterol levels.
High cholesterol levels don't cause heart disease.
Statins do not protect against heart disease by lowering
cholesterol --when they do work, they do so in another way.
The protection provided by statins is so small as to be not
worth bothering about for most people (and all women). The reality is that
the benefits have been hyped beyond belief.
Statins have many more unpleasant side effects than has been
admitted, while experts in this area should be treated with healthy skepticism
because they are almost universally paid large sums by statin manufacturers to
sing loudly from their hymnal.
Many major studies show that cutting back on saturated fats
makes no difference, and is more likely to do harm. The conclusion is that
saturated fat showed no relationship with cardiovascular disease in men.
Among the women, cardiovascular mortality showed a downward trend with
increasing saturated fat intake. In other words, the more saturated fat,
the less chance of dying from heart disease. Low cholesterol levels
greatly increase your risk of dying younger.
A detailed discussion of cholesterol research appears
in an article published by The Weston A. Price Foundation entitled "The Benefits
of High Cholesterol" by Uffe Ravnskov, MD, PhD.
He discusses a number of studies, well footnoted, which
should make those people with high cholesterol quite pleased. It is much
better to have high than low cholesterol if you want to live to be very old.
If you are taking medications to lower your cholesterol
levels, it would be worth your while to do a little research on this subject and
discuss it with your doctor because many of the medications have side effects
which are likely more dangerous than your cholesterol level.
http://www.dailymail.co.uk/pages/live/articles/health/healthmain.html?in_article_id=43068d2&in_page_i
http://www.westonaprice.org/moderndiseases/benefits_cholest.html
Return to Index
JULY
2006
ABUSE OF WOMEN IN SCOTLAND
In the June 20,
2006, edition of The Scotsman, Lyndsay Moss reported that a 36-year old
Scots mother elected to have her breasts removed and a hysterectomy after being
told she would have to wait at least two more years for the results of genetic
tests to discover if she had an increased risk of cancer. The woman has already
been waiting for 4 years for the test.
She is not alone. The backlog of women waiting for
results has been blamed on lack of funding and trained staff, changes to the way
National Health Service (NHS) services are delivered and delay in getting
licenses to carry out the tests, which have to be obtained from genetics
watchdogs. The wait in Britain is much longer.
In Scotland, some women chose to pay for private tests, at a
cost of about 1800 pounds, to get test results in weeks rather than years.
About 5% of breast cancers diagnosed each year are due to
inherited faulty genes linked to a strong family history of the disease. A
further 1- to 15% occur in women with a moderate family history of breast
cancer. Women who carry the faulty genes face a lifetime risk of
developing breast cancer of up to 85%, and up to 40% for ovarian cancer.
Many of those who test positive for the faulty genes decide
to have a preventive mastectomy and/or hysterectomy to avoid the disease.
Apparently, the women who are stuck in the National Health Service system have
to play Russian Roulette with their lives while they wait for tests.
Let's make sure that only those people who want to place
their lives in the hands of a government run health system have to do so.
All of you who are interested, form a line on the Left.
Return to Index
MAY 2006
NATIONAL HEALTH SERVICE STILL FAILING
A scathing
report by three British Government inspectorates, entitled Living Well Into
Later Life, published on March 27, 2006, and featured the same day in The
Independent, concluded that the nation's elderly are being neglected, poorly
treated and marginalized by the country's National Health Service (NHS) system.
Many older patients went hungry because meals were taken away
before they could eat them, while others suffered embarrassment through being
cared for on mixed-sex wards. There were also frequent complaints about
dirty wards, the strong smell of urine from unemptied bottles and people waiting
on trolleys.
The report says: "There is still evidence of ageism across
all services. This ranges from patronizing and thoughtless treatment from
staff, to the failure of some mainstream services such as transport to take the
needs and aspirations of older people seriously. Many older people find it
difficult to challenge ageist attitudes and their reluctance to complain can
often mean that nothing changes."
Two days earlier, the London Times Online reported
that the NHS was telling patients with multiple sclerosis (MS) they could not
have drugs to prevent their disease from getting worse because the NHS cannot
afford them.
Ministers in the British government have insisted that staff
layoffs and hospital deficits have had no effect on patient care. But a
consulting neurologist, Mike Boggild, from the Walton Centre in Liverpool, says
he knows of 50-100 MS patients who have been told they cannot have the drugs,
even though under an agreement reached in 2002 ministers promised thy would be
provided to all those who qualified.
The Department of Health said: "We have been assured they are
trying to get the drugs to new patients in Staffordshire as soon as they can."
Keep these stories in mind when politicians promise you that
if only the government ran all of the health care, everything would be
wonderful.
Return to Index
DECEMBER
2005
GOOD NEWS ON FAT
 In the
November 8, 2005 edition of Tech Central Station, John Luik brings us
some rare good news on fat.
In the
November 8, 2005 edition of Tech Central Station, John Luik brings us
some rare good news on fat.
Research present at the recent annual conference of the North
American Association for the Study of Obesity (NAASO), which was held in
Vancouver, British Columbia shows that much of what passes for obesity science
has a large element of junk science in it, such as the 400,000 Americans who die
from being overweight each year (false), or the claim that consumers of French
fries are likely to get cancer from acryl amide (false).
Studies question the claim that school vending machines are
responsible for making kids fat and should be banned. Four groups were
compared, one didn't use it at all or bought only water, one group bought 1-3
items, another 4-6, and the last, more than 6, all in the previous 30 days.
Comparing body mass index (BMI) and calories, found no difference between the
groups. The authors concluded: "Results suggest that frequency of purchase
from school vending machines was not associated with BMI percentile or DQ (Diet
Quality)."
Another study tested the theory that portion sizes in
restaurants make people fat. What they found was that portion size made no
difference in the amount of food consumed. Participants who had received
large portions did not eat more food than participants who had received small
portions, even though their portion contained five times more food.
These two studies only confirm previous research. A
recent Canadian study that looked at the eating habits of 4,298 school children
found that eating in a fast food restaurant was not a statistically significant
risk factor for obesity, even for children who eat in these restaurants more
than three times a week. It also found that there was not a statistically
significant difference between the quantity of soft drinks consumed by children
attending schools that did not sell soft drinks and those that did. It
also concluded that there was no association between the availability of soft
drinks and schools with vending machines and the risk of children becoming
obese.
He concludes: "In short, these three studies provide good
reasons to reject not only the soft drinks + vending machines = obesity theses,
but also the claims of the fat police that portion sizes promote obesity."
And coming in the same week that the US House of Representatives passed the
Personal Responsibility in Food Consumption Act by a margin of 306-120, which
would prevent the country's trial lawyers from suing restaurants and the food
industry for allegedly making people fat, it was all in all a good week for
sound science in the service of responsible public policy."
Return to Index
JULY 2005
CANADA'S FOUR-TIER HEALTH
SYSTEM
Mindelle Jacobs,
in The Edmonton Sun, on June 11, 2005 commented on the recent Canadian
Supreme Court's ruling that allowed Canadians to purchase private health
insurance.
There are many in Canada who object to the ruling on the
grounds that it could threaten Canadians' equal access to treatment.
However, there is not equal treatment under the present
system. Military personnel, the RCMP, prisoners and workers' compensation
claimants do not fall under the Canada Health Act and get speedy access to
treatment.
Since most Canadians wait and wait for a diagnostic test or
surgery, a New Brunswick man figured a way around the cue. He told police
he was planning a shooting rampage and was jailed for three years. He
actually wasn't going to hurt anyone. The 44-year old man, with no prior
criminal history needed heart surgery. He got it quickly while in custody.
Injured workers don't wait. While the average person
waits months or years for an MRI, an injured worker received one in two days
because the worker receives wage benefits when he is off work. The same is
not true of a mother with children.
The first tier of recipients are those who are wealthy enough
to go abroad for treatment.
The second tier is composed of the special classes of people
which were previously discussed.
The third tier is composed of people who have pull or
influence -- they know a doctor or have a friend on the hospital board.
The fourth and last tier are average Canadians who need care
but have no way of expediting the process.
The senior health policy analyst with the Fraser Institute,
Nadeem Esmail argues that instead of suspending the priveleges that have been
bestowed on certain groups, all Canadians should have the option of buying
health insurance.
What a novel idea.
Return to Index
MARCH
2005
IF YOU DON'T WANT TO GO TO
ASSISTED LIVING. . .
 John McCaslin, in
his February 3, 2005 "Inside the Beltway" column in The Washington Times,
recalled that in a previous column he noted that it costs just about the same
for an 80-year-old American to live out his or her days on a luxury cruise ship
($230,497) as in an assisted-living facility ($228,075). It generated
considerable response --
John McCaslin, in
his February 3, 2005 "Inside the Beltway" column in The Washington Times,
recalled that in a previous column he noted that it costs just about the same
for an 80-year-old American to live out his or her days on a luxury cruise ship
($230,497) as in an assisted-living facility ($228,075). It generated
considerable response --
"On our October cruise on Royal Caribbean lines, there was an
elderly lady who actually resided on the ship 'Voyager of the Sea," wrote Becky
Jackson-Turner of Acworth, Georgia.
"Medicare took care of her medical needs, which were few, and
whenever the ship would pull in to its main port, she would disembark for a few
hours. . . .
"She told us that it was just more financially feasible to do
this than living in an assisted-living home and was much more fun. She got
to meet new people all the time, always had great food and always had her bed
turned down for her when it was time to sleep -- with a mint to boot.
"We were blown away, but even more so when she told us of at
least 20 other people she knew who did the same, except a lot of them change
ships every once in a while to add a little variety."
Return to Index
AUGUST
2003
HEALTH CARE FORUM
By Maureen Rudel
I received a letter from Rep. Dale
Sheltrown advising me that he and Congressman Bart Stupak (both Democrats) will
be holding the Northern Michigan Health Care Forum in Ogemaw County's Horton
Township Hall on August 22, 2003 from 9 a.m. to noon.
The forum will be an open discussion of
the problems with the delivery of health care, focusing on group coverage for
small businesses and other small groups, prescription drugs, the working
uninsured and Medicaid/public health funding.
Members of local government, health
care specialists, business owners, workers and other interested members of the
public are welcome to attend and discuss potential solutions.
If you are interested in attending or
would like further information, contact Rep. Sheltrown at toll-free
1-888-347-8103.
Here is my response:
Thank you for inviting me to the forum that you and Mr. Stupak
will be having on August 22, 2003. Unfortunately,
I will be unable to attend.
I would ask that you consider my
views in your further dealing with the issues you raised.
It is of great importance to both my husband and I, since we pay for our
own health insurance without the benefit of any contribution from anyone else.
First, I would ask that both the
state and federal governments recognize medical savings accounts for all
taxpayers, without requiring that they be exhausted every year or spent on any
particular kind of insurance policy or expense. If we could put money into an account which could be used to
pay premiums (without having to meet some percentage of our income), we could
spend it as we thought best for us. If
we didn’t spend it in one year, we could continue to accumulate it to expend
on medical expenses in our later years when we will probably have more of them.
As long as the money was in an account or used for medical expenses or
insurance, it would not be taxable.
Next, if individuals had the
right to form groups for the purchase of insurance without being a member of a
certain group, i.e. lawyers, farmers, members of the chamber, etc. then the
rules of large numbers could be applied to provide actuarially sound rates which
would most probably produce lower rates.
Don’t require every policy to
be a Cadillac. Senior citizens
should be able to buy an insurance policy which does not provide maternity
coverage. Every time a politician
hears about a problem, he passes a law.
In Lansing, this year, a bill
was passed to prevent insurers from offering lower rates to lower risks.
This was done specifically at the request of Blue Cross, which has over
50% of the business in Michigan. They
didn’t like it that some other insurers offered policies at lower rates to
people who had lower risks. This
was a stupid bill. It now requires
insurers to offer rates which are within a set range.
It will raise the cost to those young people who present lower risks.
Now, instead of buying a cheap insurance policy, they will go without.
This is real progress.
In Washington D.C., a law was
passed requiring that new mothers must be allowed to stay overnight, whether
they needed to or not. This
increased the cost of coverage.
Now the Washington politicians
are trying to require that all insurance policies provide the same coverage for
mental health problems as for physical problems. This will unbelievably increase the cost, unless insurers
decide to lower the physical benefits.
Why does everyone have to have
the same policy? That is not
required for home owners policies and shouldn’t be required for health
policies. In general, medical
policies cover too much. Homeowners’
policies do not cover window washing, new carpets, or normal maintenance. They are designed to cover the catastrophic losses which
normal families cannot absorb. Health
policies should do likewise.
If many of the lab tests, normal
exams, etc. were not covered by insurance, the providers would not have to
process the paperwork which goes with the claims. That would actually cost less and could be reflected in the
cost to the customer.
I actually approve of the bill
which is working its way through Congress which will allow reimportation of
prescription drugs. I do not have
any great faith in the FDA and noting that a bunch of pharmacists in Florida
were just charged with adultering drugs and selling them, it is clear that this
risk exists. I am a great believer
in the “buyer beware” theory of marketing.
Letting people buy from whomever they wish, whatever they wish, wherever
they wish is freedom. We don’t
need the “nanny state” telling us about which drugs we should take and where
we can buy them. Underwriters
Laboratory is not a government institution and privately tests and approves
electrical devices.
I don’t believe that the poor
drug companies will stop developing new drugs.
What will probably happen is that the drug companies will raise the price
of their drugs to Canada, Germany, France and all those socialistic countries
that have socialized medicine and try to avoid the uncertainties of the
marketplace.
You raise questions about
Medicaid and Public Health funding. First,
when you provide anything for “free” there is no limit to demand.
I don’t care how poor people are, they should be required to pay
something for their health care. Perhaps,
people will choose one less color television, one less pack of cigarettes, one
less movie, to pay a dollar or two for a doctor visit.
Also, one might think a little bit before running to the doctor for every
sniffle.
If the government got out of the
business of fixing prices, prices would fix themselves.
Right now, if you go to a doctor, he never knows the cost of any
procedure or medication he recommends. This
is because he doesn’t set the price and there is no comparison shopping.
You wouldn’t accept this from an automobile dealer, and we shouldn’t
have to accept it in health care.
If we just got the government
out of the business of trying to run the health market, we would be better off.
If we were able to actually let
a market develop for senior citizens by the time that I reach 65, I would be
very grateful. I dread having to be
forced into medicare. Please find
out if Mr. Stupak will have to go into medicare when he gets to be 65.
I surely hope that if the
Congressmen and Senators have left themselves a way to opt out of that system,
they wouldn’t think twice about providing the same benefit to the people who
hire them.
Return to Index
MAY
2003
SCHIZOPHRENIA AND TEEN
BRAINS
A
little noted study published in the September 25, 2001 issue of the Proceedings
of the National Academy of Sciences commented on the use of a powerful new
analysis technique by UCLA brain researchers which shows how a dynamic wave of
tissue loss engulfs the brains of schizophrenic patients in their teen-age
years.
"This is the first study to visualize how
schizophrenia develops in the brain," said Paul Thompson, an assistant
professor of neurology at the UCLA School of Medicine and the study's chief
investigator. "Scientists have been perplexed about how schizophrenia
progresses and whether there are any physical changes in the brain. We were
stunned to see a spreading wave of tissue loss that began in a small region of
the brain. It moved across the brain like a forest fire, destroying more
tissue as the disease progressed."
Using a new analytical technique to read magnetic
resonance imaging (MRI) scans of teens as they developed schizophrenia, the
scientists noted a loss of gray matter which began in the parietal, or outer,
regions of the brain, and then spread to the rest of the brain as the disease
progressed.
The researchers are applying this technique for
diagnostic purposes. Future medications might fight the rapid loss of
brain tissue, and their effectiveness could be assessed using the imaging
technique.
Return to Index
OCTOBER
2002
BE
CAREFUL WHAT YOU WISH FOR
Once again, it is election time.
Once again, the Liberals castigate the Republicans over "universal health
care." Once again, they rail over the failure to provide
"free" medical care and prescription drugs for everyone. While
it can be argued that those who cannot afford to buy their prescriptions should
be assisted in some way, the actual number of those people is relatively
low. We continue to hear that 40 million Americans don't have access to
health care. That statement is a lie. By law, hospitals must treat
those who show up regardless of means. What is true is that at sometime
during any given year, some number of Americans are without health
insurance.
The poor have Medicaid. Many
people have insurance through their employment. Many young adults who can
afford it, choose not to buy it because they are immortal and would rather have
a new fancy car. Some who are very wealthy do not carry insurance because
they can pay for anything they need out of their own pockets. Some people
go for a short amount of time without insurance as they change jobs. There
is no health insurance crisis and never has been. However, if we don't
have a crisis, how can one introduce socialized medicine to America? Don't
you know that we are "only industrialized nation in the free world without
universal health care?" Just because the rest of these nations
have made a big mistake does not mean we should follow. Most of Europe is
Socialist to one degree or another. The Democrats want the same for us.
On January 26, 2002 The Telegraph
(UK) reported on the story of Rose Addis, a 94-year old woman who had shown
up in a hospital emergency room with a head wound from a fall. She was
found by her daughter in a chair in her emergency room cubicle 48 hours later,
confused, unwashed, and still wearing the clothes she had arrived in, now caked
with dried blood. Her family complained to the press.
In an article on the same date in the New
York Times the complaints were featured. It stated:
"Unfortunately for Mr. Blair's Labor government, such accounts are a dime a
dozen these days (though they rarely take on the dimensions of this case.)
The National Health Service (NHS) is universally acknowledged to be underfunded
and overstretched, and the chief complaints against it include neglect of
elderly patients and long, doctorless waits in squalid emergency rooms."
In response to the complaints, The
Telegraph reported that Downing Street declared war on patients who make
high-profile complaints about mistreatment in NHS hospitals. It made
public Rose Addis' medical conditions and treatments. Mr. Blairs's
spokesman made clear that the Government was no longer prepared to sit back and
allow public perceptions of the NHS to be conditioned by reports of
failures in the treatment of individual patients. He said that hospitals
and doctors should be able to "come out fighting" and put their side
of the story when their professional integrity was attacked.
The Scotsman, in an article on
August 30, 2002 reported that NHS patients waiting for treatment were
increasing. The average patient waited 57 days for treatment.
Waiting lists are currently covered by a guarantee that the maximum wait for
in-patient treatment will be 12 months, which is supposed to fall to 9 months by
the end of the year. The guarantee only covers the time between seeing a
specialist - who diagnoses what treatment is needed - and the time the treatment
is given. It does not included the time time the patient has waited to see
the specialist after being referred by a GP. The average wait for an
outpatient appointment after referral stands at 55 days.
The Christian Science Monitor,
on August 28, 2002 reported on the problems in the Canadian system. It is
the last industrialized nation to rely solely on government funds for its core
healthcare system. "We are no longer the model," said Michael
Walker, executive director of the Fraser Institute, a public-policy think tank
in Vancouver. "When you consider that equal access in a country as
spread out as Canada would require a greater number of physicians and diagnostic
equipment, we're clearly headed in the wrong direction."
Because of a lack of high-tech
equipment, wait time for diagnostic assessments can run well over three
months. The strains on the system are already forcing local shifts to
alternative models. Some communities are allowing nurses to treat minor
cases without referring patients to a doctor. 77% of the nurses and 60% of
the doctors support this approach.
Canadians are divided over the
establishment of user fees. A royal commission has been established to fix
the deficiencies. Solutions would likely include greater home care, user
fees for patients who can afford them, and private or semiprivate
hospitals. Should the commission fail to deliver a workable solution,
Canada's 10 provinces might be forced to take matters into their own hands.
Just remember, when the government
controls all of the health care, the government will decide who will get
treatment, when it will happen, and how much will be available.
Be careful what you wish for. . . .
Return to Index
AUGUST
2002
POT
AND SCHIZOPHRENIA
On July 1, 2001, UPI Science News
reported on a Japanese study which tied genetic anomalies with
marijuana-activated brain chemicals. "This result provides genetic
evidence that marijuana use can result in schizophrenia or a significantly
increased risk of schizophrenia," said lead researcher Hiroshi Ujike, a
clinical psychiatrist at Okayama University.
Schizophrenia is one of the greatest
mental health challenges in the world, affecting roughly one of every 100 people
and filling about a quarter of all hospital beds in the US. For years,
clinical scientists have known that abusing marijuana can trigger hallucinations
and delusions similar to symptoms often found in schizophrenia. Using pot
before age 18 raises the risk of schizophrenia six-fold.
The hallucinogenic properties of
marijuana are linked to a biochemical found abundantly in the brain. The
cannabinoid receptor protein studs the surfaces of brain cells and latches onto
the active chemical within marijuana known as THC.
The researchers examined the gene for
the marijuana receptor in 121 Japanese patients with schizophrenia and an
average age of 44. When they compared the same genes in schizophrenics and
148 normal men and women of the same average age, they found distinct
abnormalities in the DNA sequences among schizophrenics.
It appears malfunctions in the brain's
marijuana-linked circuitry may make one vulnerable to schizophrenia. This
holds especially true for a condition called hebephrenic schizophrenia, which is
marked by deterioration of personality, senseless laughter, disorganized thought
and lack of motivation.
There is no evidence yet these genetic
abnormalities can affect how the marijuana receptor actually acts in the
brain. The scientists would like to replicate their findings with
different ethnic population and more people.
The research is described in the
scientific journal Molecular Psychiatry.
Return to Index
MAY 2001
NO
QUICK FIX FOR PARKINSON'S
A study published in the New England
Journal of Medicine was reported in the Guardian Unlimited on March
13, 2001. The first full trial of the technique of implanting fetal cells
into the brain produced devastating results in some patients which can not be
undone.
The American scientists who conducted
the research found the therapy did not benefit patients over the age of 60 at
all. Some of the younger patients did improve, but for 15% of those who
received the implants, the outcome was worse than the disease.
The fetal cells which were implanted to
produce dopamine, the chemical that is depleted in Parkinson's sufferers, went
into overdrive. The cells appear to have grown too well and are producing
excessive amounts of the chemical causing the patients to writhe, jerk their
heads uncontrollably and throw their arms about involuntarily. The
scientists have no way of bringing the dopamine levels back down.
Paul Greene, a neurologist from the
Columbia University College of Physicians and Surgeons in New York, who was one
of the researchers, said the results were "absolutely devastating" for
the five patients who cannot control their movements.
Dr. Greene says the technique must go
back to the laboratory. "No more fetal transplants," he
said. "We are absolutely and adamantly convinced that this should be
considered for research only. And whether it should be research in people
in an open question."
The surgery in the study was carried
out at the University of Colorado School of Medicine in Denver, while the
evaluation was done in New York.
Return to Index
NOVEMBER
2000
MORE
NEWS ON SOCIALIZED MEDICINE
As we listen to Al Gore promise the
world on a silver platter, let's take another look across the pond where
socialized medicine has been around long enough to get it right, if it were ever
possible.
The Times of London reported on
July 13, 2000 that more than 80,000 cancer patients have been denied vital drugs
because the National Health Service (NHS) cannot afford them. The
Department of Health said that its cost effectiveness watchdog, the National
Institute for Clinical Excellence, would undertake an intensive program to
decide which cancer drugs should be used by the NHS. However, specialists
fear that if the National Institute for Clinical Excellence decides against new
drugs on cost grounds, it could be banning effective, life-saving treatments
that could save lives for all patients in Britain.
Are you sure Al Gore's government run
drug program is a good idea?
How about hospitals?
The Electronic Telegraph reported
on August 8, 2000 that the number of people in England waiting to see a
consultant for more than three months rose to approximately 1,091,000
people. The Department of Health immediately blamed seven hospitals which
it deemed to be a major part of the problem. The named hospitals will come
under a new "traffic light" scheme which meant that they would be
subject to more central control and conditions.
When was the last time more than 1
million Americans (with a much larger population) were waiting to see a
consultant?
It is not just England. The
Washington Times National Weekly Edition reported in the June 5-11, 2000
issue that Canada has a major problem. Canada's best graduate doctors and
nurses are moving in droves to the US because of the wages and working
conditions. In order to try to staff their medical facilities, they are
bringing in immigrants to fill the void. However, the best and the
brightest of those, in time, seek their green cards and head to the US as well,
seeking higher wages and lower taxes.
The problem with physicians and nurses
has become a crisis in British Columbia this summer. The Vancouver Sun,
September 12, 2000 reported in related stories that specialists have withdrawn
their services because of an ongoing battle over funding with the province's
health ministry. One of the problems is a lack of operating room
time. When private clinics offered to rent blocks of time in their
facilities to help with the immediate problem. David Levi, chair of the
Vancouver/Richmond Health Board refused to consider the offer. "Once
you open the window [to private delivery of medical care] you can't close
it." He believes that waits will only increase in the public system
because doctors and nurses will prefer working in the private system, where they
may get more money.
How about this? Al Gore should
move to Canada or England rather than bringing socialized medicine to us.
Return to Index
OCTOBER
2000
GORE
PEDDLES FALSE HOPES TO SENIORS
On August 27, 2000, U.S. Senator Bill
Frist, a Republican heart surgeon from Tennessee, said: "When seniors look
at the fine print of Al Gore's prescription drug plan, they're going to be very
disappointed."
According to the Kaiser Family
Foundation ["The Medicare Program," March, 2000] and the Congressional
Budget Office, the average senior spends $673 a year on prescription drugs.
The Gore prescription drug plan
requires seniors to make a 50% co-payment to cover the cost of their drugs, or
$366 for an average senior (50% of $673). In addition, the Gore proposal
requires seniors to pay a new monthly premium of $24 or $288 a year. That
means an average senior will pay $654 ($366 + $288) to receive $673 worth of
prescription drugs, leaving them with a benefit worth only $19 a year, or five
cents a day.
"We should allow seniors to choose
a program that fits their health care needs and not be forced to choose a
one-size-fits-all plan where seniors pay more into the system than they get back
in a benefit," Frist said. He recommended that instead of providing
false hope, Gore would serve the nation better by working with him and Sen. John
Breaux (D.-LA) to implement the bi-partisan plan to reform Medicare with a
prescription drug benefit.
Return to Index
AUGUST
2000
PRESCRIPTION
DRUG PLANS
The prescription drug benefit plan
proposed by the Republican Leadership Coalition and recently introduced by Sen.
Bob Smith (R-NH) and Sen. Wayne Allard (R-CO) is overwhelming preferred to that
proposed by the Clinton-Gore administration, Zogby International reported
on May 1, 2000.
The Republican plan proposes a
voluntary prescription drug benefit that would begin next year and cover 50% of
up to $5,000 in drug prescriptions per year. There would be no increase in
the Medicare premium. There would be a new combined $675 deductible that
would count toward all hospital, doctor and prescription costs toward the
deductible. The cost to the Medicare Trust Fund would be zero.
A survey of 570 Independent voters and
519 respondents over 65 (some being both) had a margin of error of 3.2%.
Of these, 68.2% supported the Republican plan and 18.8% opposed it.
The Clinton-Gore plan would begin in
2003 and cost $26 per month. It would pay 50% of up to $2,000 in
prescriptions per year. By 2009, seniors would pay $15 per month for up to
50% of $5,000 in prescriptions per year. The $100 deductible would stay
the same. It is estimated that the cost to the Medicare Trust Fund would
be $203 billion. Support for this plan was 27.6% and opposition was 59.3%.
Return to Index
APRIL 2000
WHO
ARE THE UNINSURED
Paul Sperry in Investor's Business
Daily, December 7, 1999 reported that contrary to President Clinton's
assertions that employers are dropping workers' health benefits, evidence
suggests that they are actually expanding them. Employer based coverage
climbed to 62% of the population last year -- and is the highest since 1987's
peak of 62.1%.
The answer may lie with young people
ages 18 to 24 -- one of the fastest growing age groups in America. Some
55% of that group went without health insurance for at least one month between
1993 and 1996. Many of them have access to campus health clinics.
Others are making the move from homes to full-time jobs.
Another explanation is that during the
1995 survey of the Census Bureau, allowances were made for households which had
at least one Hispanic member. That change could help account for the jump
in the uninsured, because the Hispanic uninsured rate is more than triple the
rate for whites.
Return to Index
MARCH 2000
FOR
THOSE WHO ADVOCATE SOCIALIZED MEDICINE
The Telegraph of the United
Kingdom reported on Dec. 6, 1999, that elderly patients in England are dying
because of an unspoken policy of "involuntary euthanasia" designed to
relieve pressure on the National Health Service (NHS).
Police and NHS are investigating 60
cases involving pensioners who died after allegedly being deprived of food and
water by hospital staff.
Dr. Adrian Treloar, consultant and
senior lecturer in geriatrics at Greenwich Hospital and Guy's, King's and St.
Thomas medical schools, said: "There are severe pressures on beds and in
order to relieve this there may be a tendency to limit care inappropriately
where you feel doubtful about the outcome. Are the elderly being served
properly? No, they are not getting what they deserve and I think they are being
sold short. I think that is becoming clearer and clearer. If old
people start to resist early discharge they are seen as an encumbrance."
Recent British Medical Association
guidelines say doctors should be allowed to authorize withdrawal of nutrition
and hydration by tube for stroke victims and the confused elderly, even when the
patient is not terminally ill.
NHS has been recently attacked on other
grounds. The flu epidemic created great overcrowding at the government run
hospitals. The Telegraph reported on Jan. 16, 2000 that NHS
patients are remortgaging or even selling their homes to pay for private
operations because of the long waiting lists. One hip replacement patient
was told it would be 15 months before he could even discuss his problems with a
surgeon and another 18 months before the surgery could be done. Another
man, 49, father of two, was told he needed a triple bypass after a heart attack
but discovered the waiting list for urgent cases was 10 months and for
non-urgent 14 months.
The Minneapolis Star Tribune reported
on Jan. 17, 2000, that Prime Minister Tony Blair acknowledged major problems
with the NHS but ruled out US-style private medical insurance as an
alternative. He took this position despite a well-publicized case of
a 73-year old woman with throat cancer whose operation was postponed 4 times
during the previous 5 weeks. The cancer has now spread to the point where
it is inoperable.
Both Mr. Gore and Mr. Bradley have
proposed variations of Socialized Medicine for America.
Who wants to be the first to sign up?
Return to Index
MARCH 1998
MEDICARE AND PRIVATE CONTRACTING
In the Balanced Budget Act of 1997 (BBA) a provision was
inserted which affected the right of doctors and patients to privately contract for
services. Until that time the Health Care Financing Administration (HCFA) had adopted a
rule that any doctor who accepted Medicare patients could not privately contract with any
patient for services which were provided by Medicare. However, over the years Medicare has
continued to reduce the amount which doctors could receive for services provided in an
effort to improve the solvency of the program. Many doctors have refused to accept new
Medicare patients because of the limitation on reimbursement.
To provide some relief for patients and doctors, the
Republicans had inserted a provision in the BBA which allowed doctors and patients to
privately contract for services which are otherwise provided by Medicare. The
Administration and HCFA were violently opposed to that provision because people might be
able to go outside the system to obtain services. It is the position of the Democrats that
people over 65 should not be allowed to leave the Medicare system for any service which is
provided by it. While the Republicans believe that senior citizens should be allowed to
make decisions for themselves, the President would not agree to sign the bill as proposed.
Therefore, a provision was placed in the bill which states
that any doctor who privately contracts with a patient for services which are provided by
Medicare must agree not to accept any funds from Medicare for a two year period after
entering into a private contract. This means that, in reality, no private contracts will
be allowed since 96% of the doctors participate in the Medicare system.
While HCFA claims that patients are allowed to privately
contract for services not provided by Medicare (for example, plastic surgery, a second
mammogram, other screening tests), there have been reports that such tests have been
denied. There are other occasions where a patient may wish to privately contract. For
example, if a particular specialist in your community is not taking new Medicare patients
and other available specialists are at a considerable distance away, some patients with
the means to pay may wish to use the doctor in their own community.
To deal with these problems, Sen. John Kyl and Rep. Bill
Archer have introduced bills, S. 1194 and H. R. 2497 which would allow patients to
privately contract if they pay the entire bill for the services and sign a written
contract setting forth the agreements and the restrictions on the contract. Both Rep.
James Barcia and Sen. Spencer Abraham have co-sponsored these bills. Senator Levin has
not. Neither of the bills allow the doctor to accept money from Medicare and charge a
patient additional amounts.
Return to Index








Revised:
 On Tuesday, Live Action’s Lila Rose
relayed a deeply disturbing story via Twitter about a California gay couple
buying a preborn child, renting a uterus…then ultimately killing the baby after
birth. Rose’s thread began with this tweet:
On Tuesday, Live Action’s Lila Rose
relayed a deeply disturbing story via Twitter about a California gay couple
buying a preborn child, renting a uterus…then ultimately killing the baby after
birth. Rose’s thread began with this tweet: It’s OK, go ahead
and admit it. Given the way 2020 has transpired, if a biblical-scale plague of
locusts descended upon our land, we would hardly bat an eyelash. I mean, what
else can happen? Answer: anything that once seemed possible only in the vivid
imaginations of the writers of fantastical dime-store shock novels or TV shows
like The Twilight Zone, Homeland, or 24.
It’s OK, go ahead
and admit it. Given the way 2020 has transpired, if a biblical-scale plague of
locusts descended upon our land, we would hardly bat an eyelash. I mean, what
else can happen? Answer: anything that once seemed possible only in the vivid
imaginations of the writers of fantastical dime-store shock novels or TV shows
like The Twilight Zone, Homeland, or 24.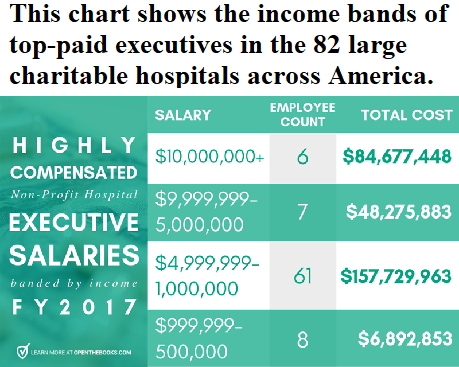
 It seems
that Michael Jacobson, watch commander of the food police and executive director
of the anti-corporate Center for Science in the Public Interest (CSPI), hates
food. On any given day, he is battling with berries, clams, fat free and fat
laden foods.
It seems
that Michael Jacobson, watch commander of the food police and executive director
of the anti-corporate Center for Science in the Public Interest (CSPI), hates
food. On any given day, he is battling with berries, clams, fat free and fat
laden foods.